Cardiomyopathy (CMP) is a generic name for various diseases of the heart muscle (myocardium). The function of the myocardium is affected, which usually leads to heart failure. The different cardiomyopathies can be classified by echocardiographic characteristics. Click here for more information about cardiomyopathy. A short review of the main characteristics for each CMP is shown below.
Differences in LV function
| Cardiomyopathy | Systolic function | Diastolic function |
|---|---|---|
| Dilated CMP | Decreased | Normal/decreased |
| Hypertrophic CMP | Increased | Decreased |
| Restrictive CMP | Normal | Decreased |
Arrythmogenic right ventricular cardiomyopathy
- Fibro?fatty replacement of the RV wall.
- Prevalence about 1 in 5000.
- Genetic component (1/3 autosomal dominant pattern, also autosomal recessive inheritance).
- Heart failure due to systolic RV dysfunction, arrhythmias and sudden death.
- Echocardiographic features:
- Diffuse or local wall motion abnormalities RV (dyskinesia).
- Systolic RV dysfunction.
- RV aneurysm basal segment near TV annulus, apical segment and RVOT.
- RV dilatation.
- Prominent trabeculation of RV.
- Increased echogenicity of moderator band.
- Relatively normal LV function and normal pulmonary pressure
- Criteria for diagnosis ARVC (ESC Task force, Eur Heart J. 2010).
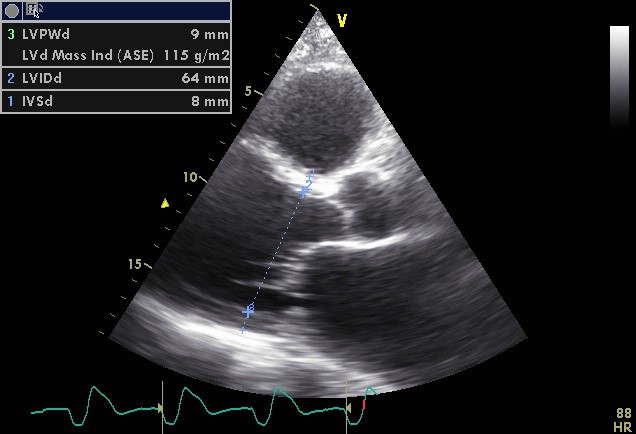
Dilated cardiomyopathy
- It is the most common form of cardiomyopathy.
- Also known as congestive cardiomyopathy.
- DCM can be inherited autosomal dominant, autosomal recessive and X-linked.
- Causes:
- Genetic.
- (Post-) infectious: various viruses and bacteria, as the final stage of myocarditis.
- Toxin and drugs: cocaine, alcohol abuse, antracycline.
- Metabolic: thiamine deficiency, hypothyroidism, hyperthyroidism, pheochromocytoma.
- Peripartum.
- Neuromuscular disease: Duchenne-Becker muscular dystrophy
- Tako Tsubo.
- Sickle cell anaemia.
- Idiopathic: No cause is found in about 30% of cases.
- Impaired LV contractility, reduced cardiac output and an increase in LV end diastolic diameter/pressure.
- It is often associated with pulmonary hypertension, dilatation of other compartments, and regurgitation of mitral and / or tricuspid valve.
- Heart failure, supraventricular arrhythmias (atrial fibrillation 20-30%), ventricular arrhythmias.
- Thrombus formation, which may lead to thrombo-embolic complications.
Hypertrophic cardiomyopathy
- Autosomal dominant inherited disease of the myocardium related to abnormalities for genes coding for sarcomere proteins.
- 60% gene mutation in sarcomere proteins.
- 5-10% other cause: Fabry?s disease, Friedrich?s ataxia, mitochondrial disease (MELAS), syndromes(Noonan, Leopard), amyloid, tacrolimus, steroids.
- Prevalence about 1 in 500-1000.
- 65% Asymmetric hypertrophy of the myocardium, usually the ventricular septum sometimes apical involvement.
- 35% Symmetrical myocardial hypertrophy (not to be confused with Aortic stenosis or hypertension).
- Small LV lumen.
- Preserved systolic LV function (EF normal or slightly decreased).
- Predominant impaired diastolic LV function.
- About 1/3 have a resting dynamic outflow obstruction and 1/3 have a provocable gradient with exercise.
- Heart failure can be caused by the rigidity of the thickened heart muscle (diastolic heart failure), by an obstruction in the LVOT (SAM) associated with regurgitation of the mitral valve. The course of the disease is progressive.
- An increased risk of thromboembolic events, sudden cardiac death due to ventricular fibrillation.
Concentric hypertrophy
Asymmetric hypertrophy
Apical hypertrophy
Non-compaction cardiomyopathy
- Also called isolated non compaction of the ventricular myocardium (INVM), a rare form of congenital heart disease.
- Spongy myocardium characterized by a thin compacted epicardial layer and a extensive non compacted endocardial layer.
- After HCM and DCM, the most common cause of primary cardiomyopathy in children.
- It is a birth defect that occurs in the 20th week of pregnancy.
- Heart failure, threatening ventricular arrhythmias, an increased risk of thrombus formation and systemic embolic events.
- Echocardiographic features:
- Prominently trabeculated myocardium with deep recesses that communicate with the LV lumen.
- Hypokinesia and myocardial thickening localized to the apex, mid-lateral and mid inferior walls.
- Ratio of the thickness of non-compacted to compacted myocardium at end-systole ? 2:1.
- Color Doppler flow showing in the recesses.
- Jenni criteria (Heart 2007).
Apical trabecularisation
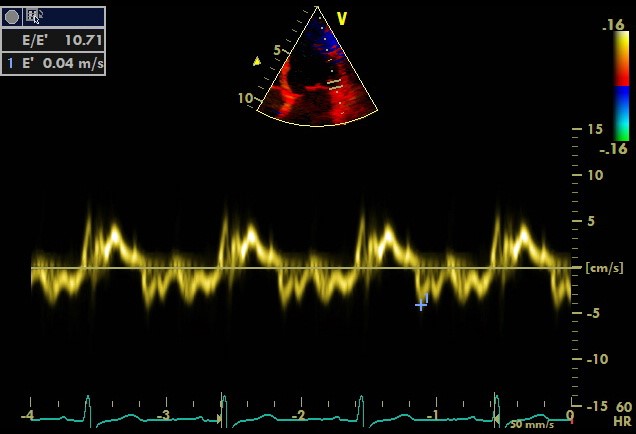
Restrictive cardiomyopathy
- Stiff and thickened myocardium.
- The 2nd most common form of cardiomyopathy and may be classified as primary (e.g., endomyocardial fibrosis, L?ffler?s endocarditis, idiopathic restrictive cardiomyopathy) or secondary. Causes of secondary restrictive cardiomyopathy include infiltrative diseases (e.g., amyloidosis, sarcoidosis, radiation carditis) and storage diseases (e.g., hemochromatosis, glycogen storage disorders, Fabry?s disease).
- Fatique, decreased exercise tolerance, right heart failure (peripheral edema, ascites).
- Echocardiographic features:
- Preserved systolic LV function.
- Non-dilated LV
- LV and RV wall thickening.
- Predominant diastolic dysfunction (see fig.).
- Biatrial enlargement.
- Pulmonary hypertension.
- Elevated RA pressure (dilated inferior vena cava).
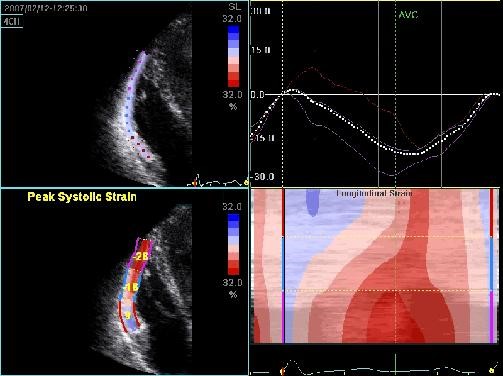
Tako-tsubo cardiomyopathy
- Tako-Tsubo is an octopus pot which is often used in Japan.
- Apical ballooning (dilatation and dyskinesia of the apex) and hypercontractile base of LV (see fig). This gives the configuration of a octopus pot.
- More prevalent in postmenopausal women’.
- Stress induced, triggered by an acute illness or intense emotional or physical stress.
- Also called ?broken heart? syndrome or ?stress cardiomyopathy?.
- Cause not fully understood. Likely multiple factors are responsible e.g. vasospasm, microvascular failure, abnormal response to catecholamines.
- Mimics an acute anterior wall myocardial infarction with ST elevations, however, without significant coronary artery disease.
- Other forms:
- reverse Tako-Tsubo ( basal akinesia and apical hyperkinesia),
- mid-ventricular type ( mid-ventricular ballooning accompanied by basal and apical hyperkinesia).
- localised type for any other segmental left ventricular ballooning with clinical characteristics of Tako- Tsubo-like LV dysfunction.
- LV function is normalized in a few days to several weeks.
The information above comes from Echocardiografie.nl. Last changed on: 20 July 2026.