The aortic annulus should be measured at midsystole from inner edge to inner edge. All other aortic root measurements (i.e., maximal diameter of the sinuses of Valsalva, the sinotubular junction, and the proximal ascending aorta) should be made at end-diastole, in a strictly perpendicular plane to that of the long axis of the aorta using the leading edge-to-leading edge (L-L) convention.
Aortic root dimensions in normal adults
| Aortic measures according to sex | |||
|---|---|---|---|
| ALL | MEN | WOMEN | |
| Aortic annular diameter, mm | 20.4 ± 2.3 | 21.2 ± 2.2 | 19.5 ± 2.1* |
| BSA-indexed annular diameter, mm/m² | 11.6 ± 1.4 | 11.3 ± 1.3 | 11.9 ± 1.4 |
| Height-indexed annular diameter, mm/m | 12.2 ± 1.2 | 12.3 ± 1.2 | 12.2 ± 1.3 |
| Aortic SoV diameter, mm | 30.8 ± 3.9 | 32.2 ± 3.7 | 29.3 ± 3.6* |
| BSA-indexed aortic SoV diameter, mm/m² | 17.6 ± 2.6 | 17.2 ± 2.5 | 18.0 ± 2.6* |
| Height-indexed aortic SoV diameter, mm/m | 18.5 ± 2.3 | 18.6 ± 2.3 | 18.4 ± 2.3* |
| Aortic STJ diameter, mm | 26.6 ± 3.7 | 27.7 ± 3.7 | 25.5 ± 3.3* |
| BSA-indexed aortic STJ diameter, mm/m² | 15.2 ± 2.4 | 14.8 ± 2.3 | 15.6 ± 2.4* |
| Height-indexed aortic STJ diameter, mm/m | 16.0 ± 2.2 | 16.0 ± 2.2 | 15.9 ± 2.2 |
| Prox. ascending ao (cm/m²) | ≤ 1,7 | ≤ 1,9 | |
Data are expressed as mean 6 SD or as number (percentage)
*P < .05, men versus women.
| Aortic Root Measurements by Age Group and Sex (WASE Study) | ||||||
| Parameter | MEN | WOMEN | ||||
| Aortic annulus (mm) | 21.5 ± 2.1 | 21.2 ± 2.2 | 20.7 ± 2.2 | 19.5 ± 1.9 | 19.5 ± 2.2 | 19.4 ± 2.3 |
| Annulus/BSA (mm/m²) | 11.3 ± 1.3 | 11.2 ± 1.4 | 11.3 ± 1.4 | 12.0 ± 1.4 | 11.7 ± 1.4 | 12.1 ± 1.6 |
| Annulus/height (mm/m) | 12.3 ± 1.1 | 12.3 ± 1.2 | 12.2 ± 1.2 | 12.1 ± 1.2 | 12.2 ± 1.3 | 12.3 ± 1.4 |
| SoV (mm) | 31.2 ± 3.4 | 32.8 ± 3.7 | 33.1 ± 4.0 | 28.1 ± 3.6 | 29.8 ± 3.2 | 31.1 ± 3.2 |
| SoV/BSA (mm/m²) | 16.5 ± 2.2 | 17.4 ± 2.4 | 18.2 ± 2.7 | 17.3 ± 2.4 | 17.9 ± 2.4 | 19.3 ± 2.8 |
| SoV/height (mm/m) | 17.8 ± 2.0 | 19.0 ± 2.1 | 19.5 ± 2.4 | 17.4 ± 2.3 | 18.6 ± 2.0 | 19.7 ± 2.1 |
| STJ (mm) | 26.7 ± 3.2 | 28.4 ± 3.6 | 28.6 ± 4.0 | 24.4 ± 3.3 | 26.0 ± 3.2 | 26.7 ± 3.0 |
| STJ/BSA (mm/m²) | 14.1 ± 2.0 | 15.0 ± 2.2 | 15.7 ± 2.6 | 15.0 ± 2.2 | 15.6 ± 2.2 | 16.6 ± 2.6 |
| STJ/height (mm/m) | 15.2 ± 1.9 | 16.5 ± 2.1 | 16.9 ± 2.4 | 15.2 ± 2.0 | 16.2 ± 2.0 | 17.0 ± 2.0 |
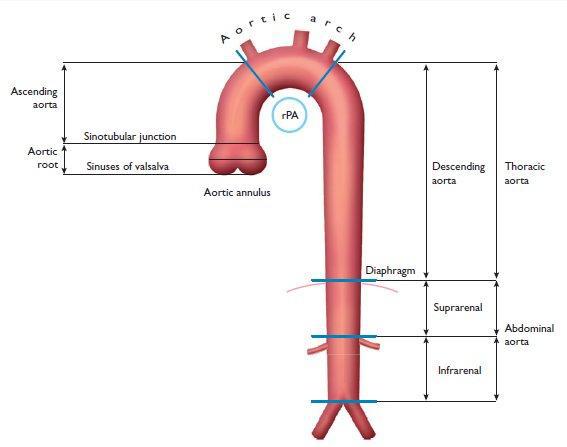
Anatomy of aorta
Ascending aorta dilation